Normal ear drum

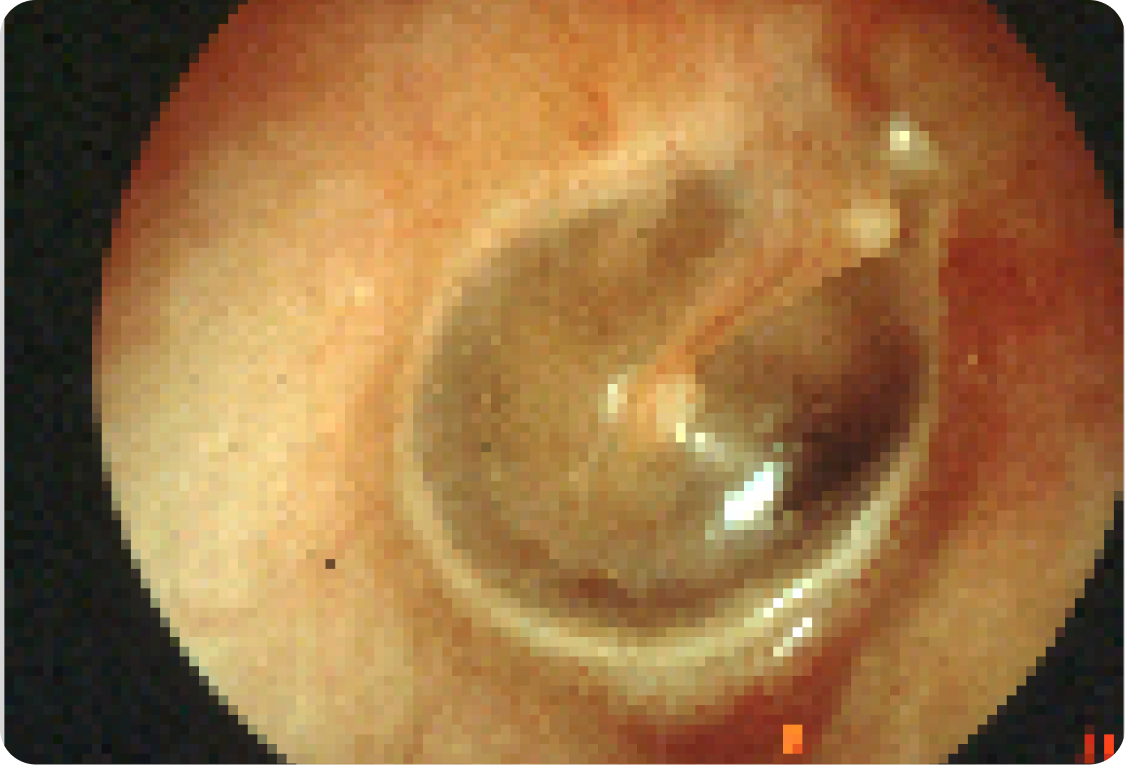
Ear infection

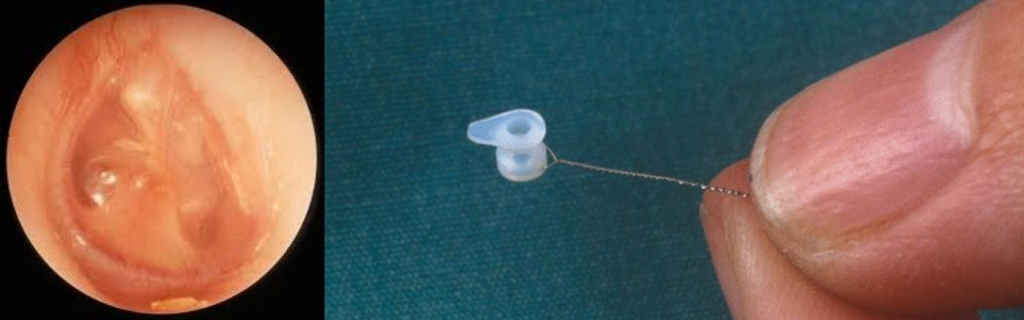
Grommets in place & eardrum back to normal

Grommets are small tubes inserted into the eardrum to drain fluid and restore normal ear function. This quick procedure helps improve hearing, reduce infections, and relieve pressure.
Grommets or ventilation tubes are placed when there has been longstanding middle ear fluid or glue. This surgery relieves the middle ear fluid therefore pressure and restores normal physiology.
Surgery in children is done under general anaesthesia and in adults under local anaesthesia. Surgery takes approximately 15 – 30 minutes and is a day surgical procedure. Children will be back to full activity the next day.
The main benefits include better hearing, fewer repeated courses of antibiotics, and relief from pressure and pain caused by ear infections.
Normal ear drum
Ear infection
Grommets in place & eardrum back to normal
Specialist ENT Surgeon
For all enquiries and appointments call (09) 925 4050
Suite A, Level 1, Kakariki Hospital
9 Marewa Road
Greenlane, Auckland 1051
Facsimile: (09) 925 4051
Only general information is provided on this web site and is not intended as advice or a consultation. Please read our full disclaimer.
Grommets are used to treat persistent middle ear fluid (glue ear), frequent ear infections, or hearing loss due to fluid buildup.
Grommets usually stay in place for 6–12 months and typically fall out on their own as the eardrum heals.
The procedure is quick and usually painless. Children undergo general anesthesia, while adults may have local anesthesia.
Swimming is generally safe, but avoid deep diving. Your doctor may recommend earplugs to prevent water from entering the ears.
In most cases, the ear returns to normal. If issues persist, further treatment may be needed.
Grommet surgery is generally safe, but risks include temporary ear discharge, a small hole remaining in the eardrum after the grommet falls out, or recurrence of ear infections.
Get in touch to book an appointment or inquire about our ENT services. Our team is here to assist you with expert care and guidance.
Otolaryngology Associates Ltd
Suite A, Level 1, Kakariki Hospital
9 Marewa Road
Greenlane, Auckland 1051
We provide expert ENT care, diagnosing and treating a wide range of ear, nose, and throat conditions. With advanced treatments and a patient-focused approach, our goal is to deliver high-quality medical care across New Zealand.

©2025 – PRIVACY POLICY – COOKIE POLICY
Made by Kickstart Digital